
The US Centers for Disease Control have concluded that a third dose of COVID-19 vaccine will be needed for protection against disease, but the science says otherwise.
A review of the immune responses to infection will help explain why vaccine boosters are not needed. The graph below shows the relative concentrations of antibody and T cells (Y axis) as a function of time after first viral infection. Antibody levels and numbers of activated T cells initially rise, then decline after the primary viral infection is cleared. Reinfections at later times (years later) are marked by a rapid immune response because of the reanimation of memory cells. The host is infected, but virus is cleared rapidly and severe disease is prevented.
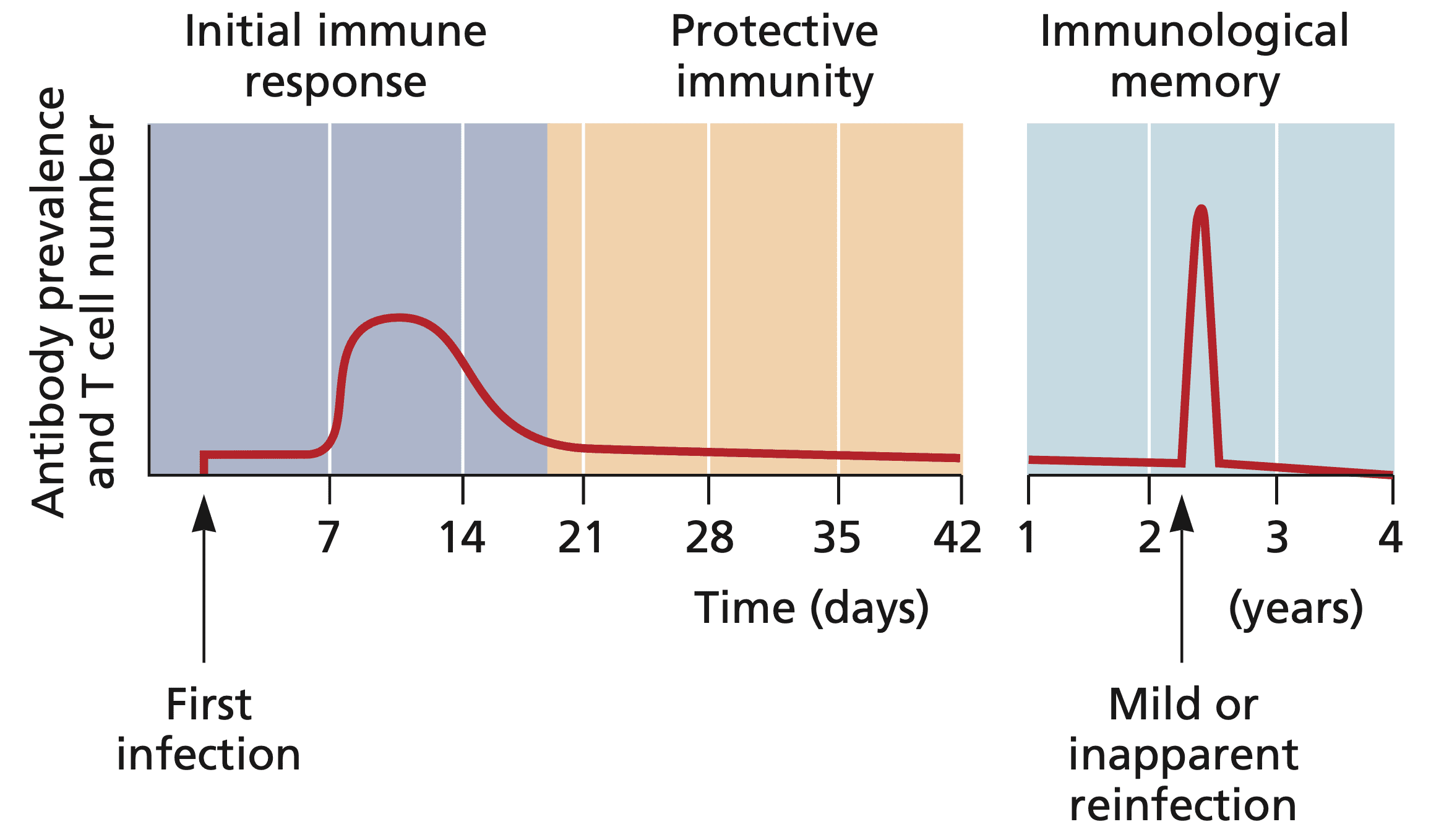
The same principles illustrated in this graph apply to the immune response after vaccination. After the first and second vaccine doses, antibodies and T cells are produced over the course of weeks and months and slowly decline to low but not non-zero levels. If a vaccinated individual is reinfected later, the memory B and T cells proliferate and virus-specific antibodies and T cells are produced. The memory response takes several days and therefore infection is not prevented. However virus reproduction in the immunized host is substantially reduced and severe disease does not occur. In addition, due to reduced viral replication in the face of a memory immune response, transmission is markedly reduced or eliminated. The impairment of transmission is the basis of herd immunity.
The COVID-19 vaccines were tested in phase III trials for their ability to prevent COVID-19 – a disease. They were not tested for their ability to prevent infection. Most human viral vaccines do not prevent infection, but they do prevent disease.
After multiple COVID-19 vaccines received emergency use authorization, studies in several countries were done to determine if immunity prevented infection. When the studies were done shortly after vaccination, antibody and T cell levels were high, and infection was prevented. But as the immune response waned (see figure above), vaccine efficiency against infection declined. This observation was incorrectly interpreted by many to indicate that the vaccines were failing. Largely ignored was the fact that vaccinated individuals were still protected from developing serious COVID-19 disease and death.
Recently public health officials in the US made the following statement:
€œThe available data make very clear that protection against SARS-CoV-2 infection begins to decrease over time following the initial doses of vaccination, and in association with the dominance of the Delta variant, we are starting to see evidence of reduced protection against mild and moderate disease. Based on our latest assessment, the current protection against severe disease, hospitalization, and death could diminish in the months ahead, especially among those who are at higher risk or were vaccinated during the earlier phases of the vaccination rollout. For that reason, we conclude that a booster shot will be needed to maximize vaccine-induced protection and prolong its durability.€
The decline of protection against infection is no cause for concern; as noted above, such a response occurs for most human viral vaccines. So that alone cannot be used to justify a third vaccine dose.
I am unaware of evidence that ‘we are starting to see evidence of reduced protection against mild and moderate disease’. Furthermore, that ‘current protection against severe disease, hospitalization, and death COULD diminish in the months ahead’ (capitals mine) cannot be used as a reason that a booster will be needed.
This week CDC released the results of two studies which demonstrate that vaccine protection against hospitalization remains strong. In one study, COVID-19 cases and hospitalizations among adults in New York were studied from May to July 2021. The results show that vaccine effectiveness against hospitalization in this state was stable: 91.9% in May to 95.3% in July. Despite increasing numbers of cases caused by the delta variant of SARS-CoV-2, hospitalization of vaccinated individuals did not increase. As would be expected as antibody and T cell levels decline, vaccine effectiveness against infection, determined by diagnostic tests, decreased from 91.7% in May to 79.8% in July.
A second study examined effectiveness of Pfizer-BioNTech and Moderna mRNA vaccines from March to July 2021 against hospitalization for COVID-19 in 18 US states. No decline in vaccine effectiveness against COVID-19 hospitalization was observed over 24 weeks: vaccine effectiveness was 86% 2€“12 weeks after vaccination and 84% at 13€“24 weeks.
These two studies provide no support for the need of a third vaccine dose in the US. If a third dose were given, the result would be an increase in virus-specific antibodies and T cells which might prevent infection for several months. But as antibody and T cell levels decline, which is inevitable, we would be in the same situation we are in now – infections occur but hospitalization and death is prevented. Would we then enter an endless cycle of giving boosters every 8 months? That is not a smart way to end this pandemic. Rather, measures to ensure that 80% of the population is fully vaccinated must be deployed.
The call for vaccine boosters in the US is another example of how some public health measures deployed during this pandemic are not based on science.
Note added after further thought: Sera from individuals who have been infected and subsequently vaccinated have broad neutralization activity against all known variants of concern. Whether boosting with existing vaccines could achieve similar breadth and potency is unknown but should be determined before giving millions of individuals a third vaccine dose.
Comments are closed.