
By David Tuller, DrPH
*October is crowdfunding month at Berkeley. I conduct this project as a senior fellow in public health and journalism and the university’s Center for Global Public Health. If you would like to support the project, here’s the place: https://crowdfund.berkeley.edu/project/22602
The pandemic has played havoc with everything, including the timeline of the development process for the new ME/CFS guidance from the UK National Institute of Health and Care Excellence. Originally, a draft of the guidance was supposed to be released earlier this year. Following a period of public comment, NICE planned to issue the final version by December. Under the new schedule, the draft version is being released in November, with a six-week comment period to follow. The final version will be released next April.
To recap: The current guidance, which was issued in 2007, recommends cognitive behavior therapy and graded exercise therapy for what was then being called CFS/ME. The committee was dominated by members the CBT/GET ideological brigades. Three years ago, NICE preliminarily decided not to revise the guidance–and then reversed itself after enormous pushback. The process of appointing the new committee took place under enormous public scrutiny. The committee ended up including both people who believe in proper science and CBT/GET ideologues, so predicting the outcome is a challenge.
In the minutes of its September board meeting, the group Forward-ME included an update from Charles Shepherd about the status of the NICE guidance development. Shepherd is the ME Association’s longtime medical director and has been involved with the process. Here’s what the minutes noted:
Charles stressed that this was going to be a completely new guideline. There had been many Zoom meetings during July and August and had made up the ground lost during lockdown. A draft with conclusions and recommendations had been produced and consensually agreed. The draft would go out to Stakeholder consultation on 10 November and there would be a 6-week consultation period ending on 22 December.
I’m not sure if that means the role of the guidance committee and its members is essentially already over. But from what I understand, NICE committee members are supposed to hold their tongues and not tweet out public pronouncements about matters that have been under deliberation. That’s why it was surprising that one member of the ME/CFS committee, Bath psychologist Jo Daniels, tweeted the following on Wednesday:
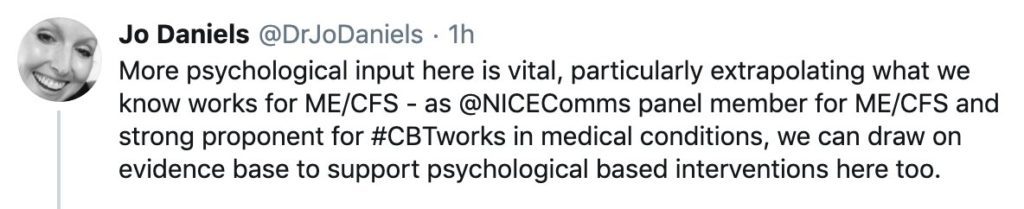
As a reminder: Earlier this year, Daniels and colleagues published a study that purported to prove the effectiveness of a specialized form of CBT for CFS/ME patients with “co-morbid severe health anxiety.” (I critiqued the study here.) Even though it is normal for patients to experience anxiety about a complex medical condition that clinicians tend to dismiss, the investigators posited it as an independent psychological problem that should be targeted for intervention. This study appeared designed to generate a funding stream for more research into “CBT-for-health-anxiety” as an treatment for anxious CFS/ME patients, but the argument disintegrated under scrutiny.
Now Daniels appears to have engaged in public advocacy on an issue before the NICE guidance committee. According to the tweet, “we know” CBT works as a treatment for ME/CFS, that is, despite international repudiation of the PACE trial and its associated treatment paradigm. The tweet has since been deleted. Maybe Daniels realized she might have crossed a line, given her position as a NICE committee member. Oops!
No worries. The tweet was captured in screen shots.
The new guidance–if it’s any good–couldn’t come soon enough, given some confusion over the applicability of the 2007 recommendations to prolonged symptoms after acute Covid-19. During the summer, NICE issued a statement warning against the assumption that the 2007 recommendation for GET also applies to patients with post-Covid symptoms. (The NICE statement did not similarly warn against CBT for post-Covid symptoms. It’s hard to read the tea-leaves, but perhaps that means GET is on shakier ground in the forthcoming draft than CBT. Or maybe not.)
Yet in a recent webinar hosted by the Royal Society of Medicine about these “long-Covid” symptoms Liverpool physician Alastair Miller cited the NICE guidance for CFS/ME in advocating GET. He did not mention the NICE advisory about this very matter. He also did not mention that NICE is developing new guidance because of widespread recognition that the one he cited in the webinar is deficient. Hey, Alastair–keep up!
Comments are closed.